

Background
Hypercoagulability is a well-known mechanism of injury in patients with COVID-19 (Rico-Mesa et al Cardiology 2020). There are several clinical reports suggesting higher incidence of venous as well as arterial thromboembolism in the infected individuals. Patients with evidence of thromboembolism are at higher risk of poor outcomes as well (Bilaloglu et al JAMA 2020). The underlying mechanism is thought to be due to increased platelet aggregation and activation (Manne et al Blood 2020) along with inflammatory activation of the coagulation cascade that can lead to a hypercoagulable state (McGonagle et al Lancet Rheumatology 2020). There is a suggestion that anticoagulation is associated with reduction in mortality in COVID-19 infections (Paranjpe et al Cardiology 2020). However, the role of antiplatelet therapy has not been very well described or studied. In this study we investigated the outcomes for patients who were on antiplatelet therapy or full dose anticoagulation at baseline who developed COVID-19 infections.
Methods
This is a retrospective electronic chart review of patients admitted to New York-Presbyterian Brooklyn Methodist Hospital (NYP BMH), a Weill Cornell Medicine-affiliated hospital in Brooklyn, NY. Patients who were diagnosed and hospitalized for COVID-19 between March to April 2020 were included. Clinical data was extracted manually from electronic medical record (EMR). Patients were divided into 3 cohorts, considered "high risk" due to chronic comorbidities which required therapeutic anticoagulation and/or antiplatelet therapy. The first cohort included patients on single or dual antiplatelet therapy (Aspirin, Clopidogrel, Ticagrelor, Prasugrel, Aspirin-Dipyridamole or dual antiplatelet therapy) prior to admission and continued on admission (AP only). The second cohort included patients on anticoagulation (therapeutic Coumadin, Apixaban, Rivaroxaban, Enoxaparin) without antiplatelet therapy prior to admission, and continued on equivalent anticoagulation inpatient (AC only). The third included patients who were on both antiplatelet therapy and therapeutic anticoagulation (AP + AC). Additionally, we collected data on baseline characteristics, demographics, and outcomes. The primary outcome of the study was inpatient mortality. Secondary outcomes were median length of stay, ICU admission, Intubation requirement, bleeding, transfusions of blood products, development of venous thromboembolism and myocardial infarction. Chi-squared analyses were performed to determine statistical significance.
Results
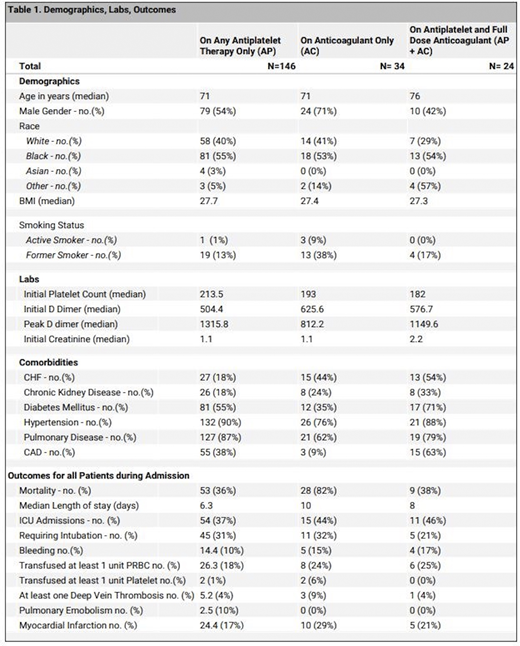
We analysed 684 hospitalized patients who were diagnosed with COVID-19. Ages ranged from 18 to 101 years old, 52% were male, and 48% were black, with a median age of 70. There were 146 patients in the AP group, 34 patients in the AC group, 24 patients in the AP + AC group, and 480 patients were on neither. Our data was significant for mortality of 82% in the AC group, 36% in the AP group, and 38% in the AP + AC group (p value <0.00001). 37% of AP patients required ICU admission, 44% of AC patients, and 46% for AP + AC patients. 31% of AP patients required intubation, 32% of AC patients, and 21% of AP + AC patients. 24% of AC patients required at least 1 unit packed red blood cell transfusion, and 25% of AP + AC patients (Table 1).
Conclusion
We determined our patients to be those at high risk of thrombosis at baseline due to their requirement of antiplatelets or anticoagulation prior to hospitalization for COVID-19 infection. Our study suggests that mortality is higher for these patients who already required anticoagulation prior to COVID infection. Significantly, we demonstrated that patients on both therapeutic anticoagulation and antiplatelet therapy had less mortality than patients on anticoagulation alone, suggesting that antiplatelets in addition to anticoagulation might be protective against mortality in COVID-19 infection. Additionally, patients on antiplatelets and anticoagulation had less development of respiratory failure requiring intubation than either alone. This study provides proof of concept for prospective clinical trials for assessing the role of combination of antiplatelet therapy and therapeutic anticoagulation in high risk patients.
No relevant conflicts of interest to declare.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal